
 Home/Blog
Home/BlogGiven the global hysteria over the spread COVID-19, you might be excused if you are very surprised to learn that the most recent week of mortality data in the EU shows an actual decline from what is expected for this time of year.
In the coming months there will be an increasing debate over whether the virtual shutdown of our economy was warranted given the threat of the latest form of the coronavirus, SARS-CoV-2. While there are still large uncertainties about how fast it spreads and how lethal it is (statistically, those are inversely related), I suspect we will ultimately realize that our response might well have done more harm than good to society as a whole.
This is mainly because poverty is the leading cause of premature death in the world, and shutting down the economy leads to premature death for a multitude of reasons related to poverty. In the extreme example, you could save lives in the short run by keeping everyone at home, but in the long run we would all starve to death.
But that is not the main subject of this post.
A couple weeks ago I started expressing the opinion on social media that if our reaction to the spread of COVID-19 turns out to be overdone, it might end up having the unexpected consequence of reducing total virus-related mortality.
Let me explain.
As I am sure you are aware, seasonal flu is a global killer, with 300,000 to 650,000 deaths on average each year, mainly among the elderly and those with pre-existing health conditions. At this writing, COVID-19 has killed 10% or less of that number. (Yes, I realize that number might have been considerably higher if not for our response).
Here’s the point: It might well be that the increased level of hand-washing, sanitizing, and social distancing we have exercised might save more lives from reducing influenza-A and -B that were lost to COVID-19, and that net virus-related mortality might go down this season.
I personally became more careful about not spreading germs several years ago. No so much for myself (I have a pretty strong immune system) but so I would not carry disease home to my family members. I carry antibacterial wipes in my car and use them religiously. We are hearing more and more now about how such habits can help prolong the lives of those around us who are elderly or have compromised immune systems.
Now, recent results from Europe suggest that the COVID-19 response might be having the unintended benefit of saving total lives. This is all very preliminary, I realize, and that coming weeks might see some change in that picture. But it is worth thinking about.
Early Results from Europe
Every week (on Thursday) the Euro MOMO project (European MOnitoring of excess MOrtality) publishes a report of mortality statistics across the EU, including stratification by age group. The latest report (which I believe includes data through March 24, but I am not sure) shows (green line) no uptick in total mortality from the assumed baseline (red line). In fact, it’s a little below that line (they also account for missing and late reports).
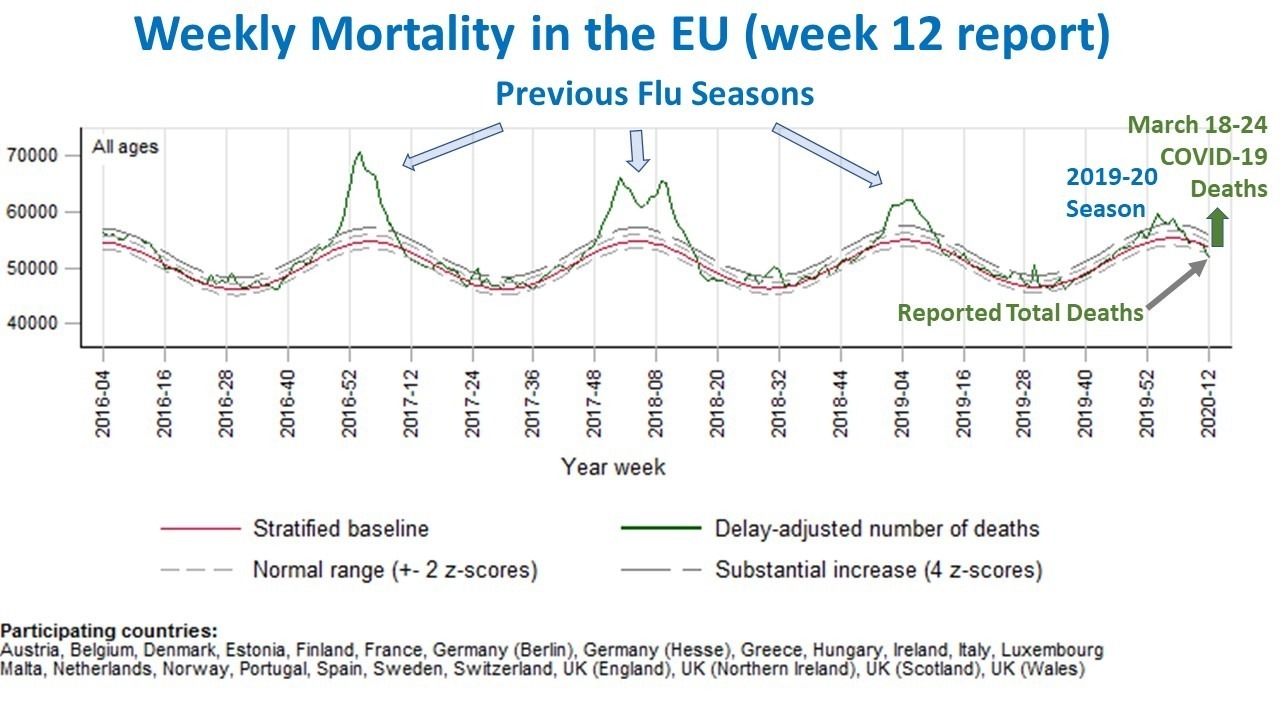
Amazingly, this flu season is seen to be surprisingly mild compared to previous flu seasons in the EU. On the chart I have also indicated the number of reported COVID-19 deaths in the most recent week, around 7,000.
Why do we not see an uptick on the chart? The charts for individual countries do show an up-tick for Italy (for example), but not unlike what was seen in previous flu seasons.
The report itself provides two or three possible explanations, none of which are particularly satisfying. Read it yourself and tell me it doesn’t sound like the people writing the report are also somewhat mystified. They don’t mention what I am discussing here.
So, the chart begs at least two questions:
1) Are the effects of practicing increased hygiene in response to COVID-19 saving more lives that would have been lost to seasonal flu deaths, than are being lost to COVID-19 itself?
2) Why are we not outraged and deathly afraid of the seasonal flu (-A and -B), given the widespread death that routinely occurs from those viruses that come around each season?
You might claim, “It’s because COVID-19 can kill anyone, not just the elderly.” Well, that’s true of the seasonal flu, as well. The case of an apparently healthy 44-year-old Texas man who recently died of COVID-19 probably scares many people, but according to the CDC approximately 5 “healthy” young people a day in the U.S. under the age of 25 die from sudden cardiac arrest. Maybe that Texas man had an underlying health condition that was previously undiagnosed. Unless they do an autopsy, and the family reveals the results, we will never know.
And, you might well think of other reasons why EU deaths have not experienced an uptick yet. Human behavior involves many confounding variables. I’m just mentioning one potential reason I am not seeing discussed.
I am not trying to minimize the deaths due to COVID-19. I’m trying to point out that if we are fearful of death from COVID-19, we should be even more concerned about the seasonal flu (many people are saying this), and that one benefit of the current experience might be that people will be more mindful about avoiding the spread of viruses in the future.

Very good blog post. I absolutely love this site. Keep it up!